Table of Contents
Introduction to Bipolar Disorders
Bipolar disorder, formerly known as manic-depressive illness, is a chronic mental health condition characterized by extreme shifts in mood, energy, activity levels, and the ability to carry out day-to-day tasks. These shifts range from depressive lows (sadness, hopelessness, loss of interest) to manic or hypomanic highs (elevated mood, increased energy, racing thoughts). It is a lifelong condition, but with proper treatment (medication, therapy, lifestyle management), most individuals can achieve stability and lead fulfilling lives. The disorder typically emerges in late adolescence or early adulthood.
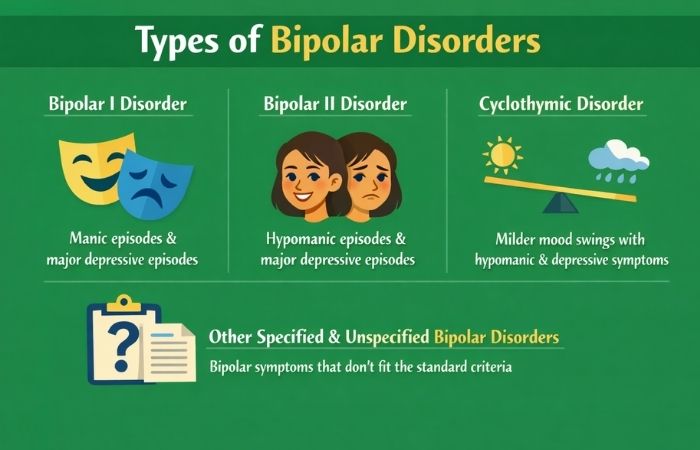
Types of Bipolar Disorders
| Type | Key Feature | Manic Episode | Depressive Episode |
|---|---|---|---|
| Bipolar I Disorder | Full-blown manic episodes | At least 1 episode lasting ≥7 days, or severe enough to require hospitalization. Depressive episodes common but not required. | Common, lasting at least 2 weeks. |
| Bipolar II Disorder | Hypomanic + major depressive episodes | Hypomanic episodes (less severe than mania, lasting ≥4 days). No full mania. | At least one major depressive episode lasting ≥2 weeks. |
| Cyclothymic Disorder | Chronic mood instability | Mild hypomanic symptoms (not full episode) for ≥2 years (1 year in adolescents). | Mild depressive symptoms (not full episode) for ≥2 years. |
| Other Specified | Symptoms that don’t fully match above categories | Short-duration hypomania, or episodes with insufficient symptoms. | Varies. |
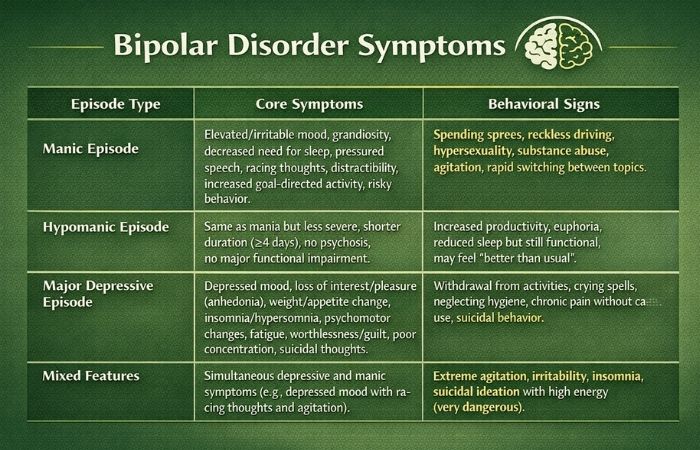
Bipolar Disorder Symptoms
| Episode Type | Core Symptoms | Behavioral Signs |
|---|---|---|
| Manic Episode | Elevated/irritable mood, grandiosity, decreased need for sleep, pressured speech, racing thoughts, distractibility, increased goal-directed activity, risky behavior. | Spending sprees, reckless driving, hypersexuality, substance abuse, agitation, rapid switching between topics. |
| Hypomanic Episode | Same as mania but less severe, shorter duration (≥4 days), no psychosis, no major functional impairment. | Increased productivity, euphoria, reduced sleep but still functional, may feel “better than usual.” |
| Major Depressive Episode | Depressed mood, loss of interest/pleasure (anhedonia), weight/appetite change, insomnia/hypersomnia, psychomotor changes, fatigue, worthlessness/guilt, poor concentration, suicidal thoughts. | Withdrawal from activities, crying spells, neglecting hygiene, chronic pain without cause, suicidal behavior. |
| Mixed Features | Simultaneous depressive and manic symptoms (e.g., depressed mood with racing thoughts and agitation). | Extreme agitation, irritability, insomnia, suicidal ideation with high energy (very dangerous). |
Key Differences Between Bipolar I and II
| Feature | Bipolar I Disorder | Bipolar II Disorder |
|---|---|---|
| Mania | Yes (full manic episodes) | No (only hypomania) |
| Hypomania | May occur but not required | Required |
| Major Depression | Common but not required for diagnosis | Required (at least one episode) |
| Psychosis | Possible during mania or depression | Rare (if occurs, diagnosis likely changes to Bipolar I) |
| Functional Impairment | Severe during mania; often requires hospitalization | Less severe during hypomania; impairment mainly from depression |
| Course of Illness | More manic episodes; can be more volatile | More depressive episodes; longer duration of depression |
Causes and Risk Factors
| Category | Specific Factors |
|---|---|
| Genetic | 80–90% heritability; risk if first-degree relative (10x higher); specific genes (e.g., CACNA1C, ANK3) implicated. |
| Neurobiological | Imbalances in dopamine, serotonin, norepinephrine; structural brain changes (reduced prefrontal cortex volume, enlarged amygdala/ventricles); circadian rhythm dysfunction. |
| Environmental | Stressful life events (trauma, loss, divorce); sleep deprivation (can trigger mania); substance abuse (cocaine, amphetamines, alcohol). |
| Psychological | High sensitivity to reward; poor emotion regulation; negative cognitive styles. |
| Perinatal | Postpartum period (high risk for mania/psychosis, especially in women with bipolar I). |
Medicine for Bipolar Disorder
| Drug Class | Examples | Main Use | Key Notes |
|---|---|---|---|
| Mood Stabilizers | Lithium, Valproate (Depakote), Carbamazepine, Lamotrigine | Long-term maintenance; acute mania (lithium/valproate); depression (lamotrigine) | Gold standard: Lithium. Requires blood monitoring (lithium, valproate). |
| Atypical Antipsychotics | Quetiapine (Seroquel), Olanzapine (Zyprexa), Aripiprazole (Abilify), Lurasidone (Latuda), Risperidone | Acute mania, mixed episodes, bipolar depression, maintenance | Often used alone or with mood stabilizer. Metabolic side effects common. |
| Antidepressants | SSRIs (fluoxetine), bupropion | Bipolar depression (controversial) | Only with mood stabilizer to avoid switch to mania. Generally avoided in bipolar I. |
| Benzodiazepines | Lorazepam, clonazepam | Short-term for agitation, insomnia, anxiety | High risk of dependence; not for long-term use. |
| Combination Products | Olanzapine-fluoxetine (Symbyax) | Acute bipolar depression | FDA-approved specifically for depressive episodes. |
Best Doctors for Bipolar Disorders – Table (Examples – U.S. Focus)
Note: “Best” depends on location and insurance. Listed are nationally recognized experts.
| Doctor | Institution | Specialty Focus |
|---|---|---|
| Dr. Michael E. Thase | University of Pennsylvania | Bipolar depression, psychotherapy + pharmacotherapy |
| Dr. K.N. Roy Chengappa | University of Pittsburgh | Mood stabilizers, treatment-resistant bipolar |
| Dr. Lori L. Altshuler | UCLA | Bipolar disorder in women, reproductive psychiatry |
| Dr. Trisha Suppes | Stanford University | Long-term outcomes, bipolar spectrum |
| Dr. Joseph F. Goldberg | Icahn Mount Sinai | Pharmacotherapy, mixed states, rapid cycling |
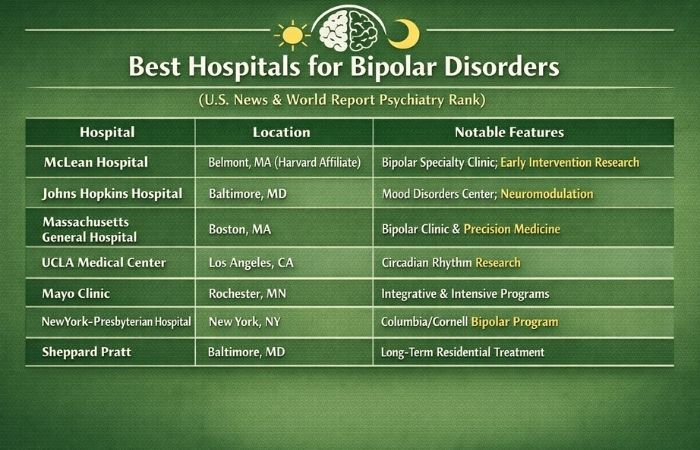
Best Hospitals for Bipolar Disorders (U.S. News & World Report Psychiatry Rank)
| Hospital | Location | Notable Features |
|---|---|---|
| McLean Hospital | Belmont, MA (Harvard affiliate) | Bipolar Specialty Clinic; research on early intervention |
| Johns Hopkins Hospital | Baltimore, MD | Mood Disorders Center; advanced neuromodulation |
| Massachusetts General Hospital | Boston, MA | Bipolar Clinic & Research Program; precision medicine |
| UCLA Medical Center | Los Angeles, CA | Resnick Neuropsychiatric Hospital; circadian rhythm research |
| Mayo Clinic | Rochester, MN | Integrative care; inpatient and intensive outpatient programs |
| NewYork-Presbyterian Hospital | New York, NY | Columbia/Cornell joint program; specialty in peripartum bipolar |
| Sheppard Pratt | Baltimore, MD | Long-term residential treatment for bipolar |
Conclusion
Bipolar disorder is a serious but highly treatable medical condition. Accurate diagnosis of the specific type (I, II, cyclothymia) is critical because treatment differs—especially the use of antidepressants, which can trigger mania in bipolar I. A combination of mood stabilizers (lithium remains the gold standard), atypical antipsychotics, and psychotherapy (CBT, interpersonal and social rhythm therapy) offers the best outcomes. With proper long-term management, including medication adherence, sleep hygiene, stress reduction, and regular follow-up with a psychiatrist, individuals with bipolar disorder can achieve stability, maintain relationships, and succeed in their careers and personal lives.
FAQs
1. Is bipolar disorder the same as mood swings?
No. Everyone has mood swings, but bipolar episodes last days to weeks and significantly impair functioning.
2. Can someone with bipolar disorder live without medication?
Highly discouraged. Relapse rates without medication exceed 70% within 1 year. Medication is the foundation of treatment.
3. Does bipolar disorder get worse with age?
If untreated, yes—more frequent and severe episodes. With treatment, many remain stable. Some experience “burnout” of mania in late life.
4. Can diet or supplements help?
Omega-3 fatty acids (fish oil) and N-acetylcysteine (NAC) have shown modest benefits as adjuncts to medication, but never as replacements.
5. Is bipolar disorder genetic?
Strongly. If one parent has bipolar, child’s risk is ~10–15%; if both parents, ~40–70%.
6. Can trauma cause bipolar disorder?
Trauma does not cause bipolar on its own but can trigger onset in genetically vulnerable individuals and worsen the course.
7. What is rapid cycling?
4 or more mood episodes per year. More common in bipolar II and women. Often requires medication adjustment.
8. How is bipolar II different from major depression?
Major depression has no hypomania. A person with bipolar II will have had at least one hypomanic episode (≥4 days of elevated mood/energy).
9. Are psychedelics or ketamine used for bipolar?
Ketamine (esketamine) is studied for bipolar depression but carries risk of mania. Psychedelics (psilocybin, LSD) are generally contraindicated due to psychosis risk.
10. Can a person with bipolar disorder hold a high-stress job?
Yes, with excellent treatment adherence, sleep regularity, and workplace accommodations. Many successful CEOs, artists, and professionals have bipolar disorder.